Fertility options before cancer treatment
There are fertility options available to you before you start treatment. It is possible for some people to have a healthy child after choosing any of these fertility options before treatment.
The most common fertility options available to you before treatment in Canada include:
- Wait and see (no fertility preservation used)
- Embryo cryopreservation (embryo freezing). An embryo is made when an egg is combined with sperm.
- Oocyte cryopreservation (egg freezing)
- Ovarian suppression (temporarily shutting off ovarian function)
Less common and experimental fertility options that may be available to you before treatment include:
- Ovarian tissue banking (removing and freezing tissue from your ovary)
- In vitro maturation (removing immature eggs from your ovaries)
Click here to learn more about the less common and experimental fertility options.
Please note: the fertility options presented may not be right for everyone. It is important to talk with your healthcare team to decide which of these options might be safe for you.
| Frequently Asked Questions | Wait & See | Embryo freezing | Egg freezing | Ovarian suppression |
|---|---|---|---|---|
| What does the fertility option involve? | 1. You start treatment without taking any steps to preserve your fertility |
Before treatment:
After treatment:
This process is called in vitro fertilization and embryo transfer. |
Before treatment:
After treatment:
This process is called egg freezing, in vitro fertilization and embryo transfer. |
Before treatment:
|
| Where is this option available? | Available to everyone | All fertility clinics | Most fertility clinics | All oncologists can give you these drugs. However, not all oncologists believe that it will work to protect your eggs. |
| Will my treatment be delayed? | No delay | Possibly - Takes 2 to 4 weeks. It may take longer for some people. | Possibly - Takes 2 to 4 weeks. It may take longer for some people. | No delay |
| What is the average cost to me? | No cost | $0 to $20,000 | $0 to $15,000 | $0 to $500 every month |
| Is there funding available? | Not applicable |
Possibly – funding may be available. Some provinces cover the costs of embryo and egg freezing. Learn about available funding by province on our Cost of fertility preservation page. Fertile Future may give you up to $2500 through the Power of Hope program www.fertilefuture.ca. Your drug insurance plan may cover the cost of drugs. Compassionate medication programs are also available www.infertilitynetwork.org/insurance |
||
|
What is my chance of getting pregnant? Your chance of having a child by your age are detailed below |
Depends on:
|
Depends on:
|
Depends on:
Freezing eggs has a lower chance of pregnancy than freezing embryos |
Depends on:
We do not know for sure that this works. |
| What are my risks? | Your treatment may decrease the number of eggs in your ovaries. You may be unable to have a natural pregnancy after treatment. |
You may be at an increased risk of:
Ask your fertility specialist about your specific risks. |
You may have menopause symptoms and reversible thinning of bones. | |
| What other factors should I consider? | You may decide to wait and see if you do not have time or money to complete another fertility option or as a personal preference. Choosing another fertility option may be stressful. Consider which decision has the most impact on future "you". You may have to wait for several years after treatment before trying to get pregnant. |
Sperm is needed to create embryos. You can get sperm from your partner and/or donor sperm. Donor sperm is available within 48 hours from a sperm bank. Counselling may be advised if you decide to use donor sperm. If you choose to freeze embryos with a stable partner/relationship, you both must agree to the future use. This means that if the relationship ends, you have lost your reproductive freedom. You alone cannot make the decision about what do with the embryos. You may face religious or ethical challenges if you do not need the embryos after treatment. Maximum storage time for your frozen embryos may vary by clinic. |
You do not need sperm at the time of egg collection or freezing. You can freeze some eggs and some embryos at the same time if you have access to sperm. Maximum storage time for your frozen eggs may vary by clinic. You maintain your reproductive freedom. You alone have the right to make decisions about what to do with your frozen eggs. |
You may decide to have ovarian suppression if you do not have time to complete another fertility option or as a personal preference. Your periods will stop when you are using ovarian suppression. You can combine this approach with embryo or egg freezing. |
What is my chance of having a pregnancy with the fertility options?
It is important to remember:
- chemotherapy reduces your ability to become pregnant and we do not know by how much exactly. It will be different for each person.
- your age when you plan to get pregnant will affect whether you have a successful natural pregnancy after treatment
- your age when you freeze eggs or embryos will affect whether you have a successful pregnancy using the frozen eggs or embryos
- even if your periods come back after chemotherapy, it does not always mean that you will be able to have a natural pregnancy
Read the information below and then find your age range chart for more information.
- Wait and see
The chance of having a natural pregnancy after treatment is based on your age and, to some extent, the type of chemotherapy that you get. Even if you do not get chemotherapy, your natural fertility decreases as you age and your chance of having a miscarriage increases.
- Embryo freezing
-
The pregnancy rates for embryo freezing are averages from 34 fertility clinics across Canada in 2015. These averages include people who froze embryos at these clinics during the course of treatment for infertility.
How many embryos will survive the thawing process? The number of eggs collected varies. The collected eggs will be fertilized with sperm. But not all eggs will successfully fertilize to create embryos. All embryos that are successfully created will be frozen. Approximately 90% of frozen embryos will survive the thawing process. The success of a frozen thawed embryo creating a pregnancy is dependent on the age of the person who produced the egg that made the embryo.
- Egg freezing
-
As this is a newer procedure there are no data on the pregnancy rates from fertility clinics in Canada. Pregnancy rates vary for each fertility clinic and you should discuss them with your fertility specialist.
How many eggs will survive the thawing process? The number of eggs collected varies. The collected eggs will be frozen. Approximately 80-90% of frozen eggs will survive the thawing process. The eggs that survive will be fertilized with sperm. But not all eggs will successfully fertilize to create embryos.
Are my chances of getting pregnant lower when I freeze eggs compared to embryos? If your eggs are thawed and fertilized to create healthy embryos then your chances of getting pregnant are the same as if you decided to freeze embryos. However as some eggs may not survive the thaw process, you may have fewer embryos created from frozen eggs than you may from fresh eggs.
You can use an online tool to estimate the chance of having a child after freezing your eggs. This calculator takes your age into account. Online tool: www.fertilitypreservation.org/contents/probability-calculator
- Ovarian suppression
We do not know for sure that ovarian suppression can protect eggs. Some studies show promising results for ovarian suppression preventing premature menopause after chemotherapy for breast cancer. However, it is not clear if it improves your chances of having a child after treatment. More research is being done to see if ovarian suppression can protect eggs during chemotherapy.
Please note: The success rates are based on people with and without cancer. We have limited information about fertility success rates for breast cancer survivors. Your chance of success depends on your individual situation. Talk with your healthcare team to understand your specific chances.
What are my chances of getting pregnant with the fertility options?
Wait and See
- What are my chances of pregnancy if I choose to wait and see before chemotherapy?
-
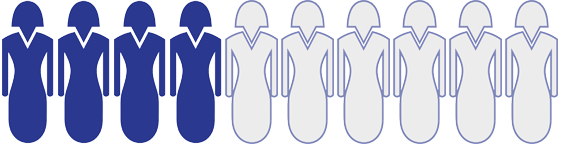
The table below shows your chances of getting pregnant by age range if you decide to wait and see. NOTE: Not all pregnancies will result in a live birth. Age range when you try to get pregnant after treatment Risk of chemotherapy affecting your fertility Chance of having a natural pregnancy in one year Under age 30 when you try to get pregnant LOW Approximately 7 out of 10 people (70%) will have a natural pregnancy in one year

30 to 34 years of age when you try to get pregnant LOW to MEDIUM Approximately 4 out of 10 people (40%) will have a natural pregnancy in one year
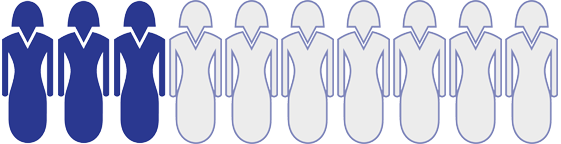
35 to 39 years of age when you try to get pregnant MEDIUM Approximately 3 out of 10 people (30%) will have a natural pregnancy in one year
40 to 44 years of age when you try to get pregnant HIGH Your chances of having a natural pregnancy are very low. They are less than 10%
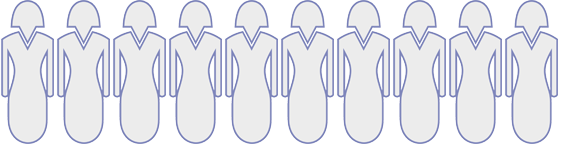
Over age 44 when you try to get pregnant VERY HIGH Your chances of having a natural pregnancy are very low. They are less than 1%
Please note: A successful pregnancy will depend more on your age when you try to get pregnant after treatment. Talk with your doctor to see how long your treatment will last and when you can safely try and get pregnant.
Embryo Freezing
- What are my chances of pregnancy if I choose to freeze embryos before chemotherapy?
-
Your chance of having a pregnancy with embryo freezing is on top of any natural ability you may have to get pregnant after chemotherapy
The table below shows your chances of having a pregnancy by age range if you decide to freeze embryos. Remember that the chance of having a pregnancy in the general population under the age of 35 is only around 20% to 30% each month. NOTE: Not all pregnancies will result in a live birth.
Age range when you freeze your embryos Chance of having a pregnancy each time embryos are put into the womb Under age 30 when you freeze embryos Approximately 5 out of 10 people (50%) will have a pregnancy each time embryos are put into the womb
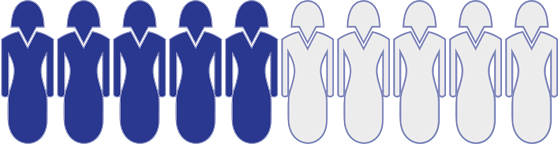
30 to 34 years of age when you freeze embryos Approximately 4 out of 10 people (40%) will have a pregnancy each time embryos are put into the womb
35 to 39 years of age when you freeze embryos Approximately 3 out of 10 people (30%) will have a pregnancy each time embryos are put into the womb
40 to 44 years of age when you freeze embryos Approximately 1 out of 10 people (10%) will have a pregnancy each time embryos are put into the womb
Over age 44 when you freeze embryos Your chances of having a pregnancy using your own eggs are very low. They are less than 2%
There are increased risks for any person who gets pregnant and has a child at an older age. Visit the Society of Obstetricians and Gynecologists in Canada for more information on the risks.
Please note: A successful pregnancy will depend more on the age when your embryos were frozen before treatment.
Ovarian Suppression
- What are my chances of my period coming back if I choose ovarian suppression before chemotherapy?
-
There is not enough research completed on ovarian suppression to separate it out by age. The chart below shows the chances of your period coming back after using ovarian suppression compared to those who did not use ovarian suppression.
Fertility Option Age range when you start chemotherapy Chance of your period coming back after chemotherapy No ovarian suppression Most people between 35 to 40 years of age Approximately 7 out of 10 people (70%) got their periods back after chemotherapy
Ovarian suppression Most people between 35 to 40 years of age Approximately 8 out of 10 people (80%) got their periods back after chemotherapy

Please note: We do not know how much ovarian suppression improves your chances of getting pregnant after treatment. We only know the chance of your period coming back after treatment. But your period coming back after treatment does not always mean you will be able to get pregnant.